Cataract surgery in challenging cases
CASE HISTORY
A 71-year-old female presented with bilateral cataracts.
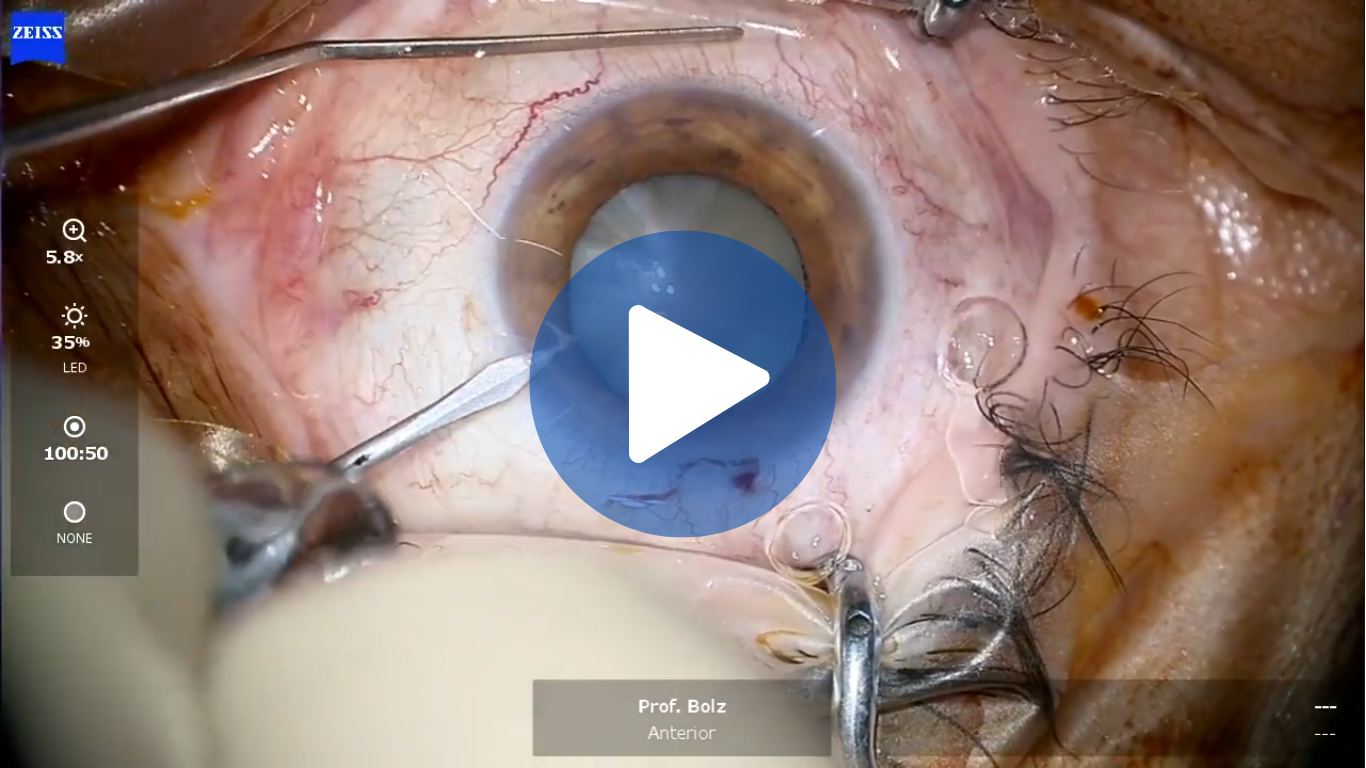
The right eye had a brunescent cataract and decimal BCVA was 0.1 (Figure 1). The fellow eye had a cataracta provecta and decimal BCVA was 0.87.
Cataract surgery was scheduled for the eye with the brunescent cataract followed 1 week later by surgery for the fellow eye. The first eye procedure was performed using the miLOOP (Carl Zeiss Meditec AG) to divide the lens into four quadrants followed by phacoemulsification of the lens and irrigation/aspiration. Lens removal was completed without any complications. Phacoemulsification time was 7 seconds. A single-piece C-loop haptic monofocal IOL was implanted. The patient was prescribed standard postoperative medication with a topical corticosteroid, antibiotic and nonsteroidal anti-inflammatory drug along with hyperosmolar eye drops as a precaution to minimize corneal edema. At examination on postoperative day 2, the cornea had minimal Descemets folds (Figure 1), which were attributable to the increased ultrasound energy needed for phacoemulsification of a dense brunescent lens but less than expected if a phaco chop technique was used for lens fragmentation. Refraction was +1.00 sph -1.50 cyl @ 95°, and BCVA was 0.4.


Fig. 1. Images of the right eye preoperatively with a brunescent cataract
and from postoperative day 2.
When the patient returned at day 7 after surgery, Descemets folds had resolved and BCVA had improved to 0.5. Because of the fast visual recovery, the patient was able to undergo the second eye surgery as planned.
DISCUSSION
Patients with a brunescent cataract are not commonly encountered outside of underdeveloped countries. When these cases present, they can pose a challenge for even the most experienced cataract surgeons. Greater phacoemulsification energy is needed to divide and remove the dense nucleus of a brunescent cataract, and surgery time can be prolonged. Consequently, these cases are at risk for increased corneal endothelial damage, corneal edema, wound burn, capsular tears and postoperative inflammation that together can contribute to delayed visual recovery and long-term corneal endothelial cell loss. For the past 12 months, I have been using the miLOOP for energy-free disassembly of the nucleus in eyes with a brunescent cataract. Consistent with results of published prospective and retrospective studies, my experience shows that using the miLOOP minimizes ultrasound energy usage. I have observed less corneal edema after using the miLOOP in cases of brunescent cataract that is associated with faster visual recovery and allows me to shorten the interval to the fellow eye surgery.